Kenichi A. Tanaka, MD, Nobukazu Sato, MD, Andrew B. Kelly, DVM, Fania Szlam, Jerrold H. Levy, MD
Department of Anesthesiology
Emory University School of Medicine, Atlanta, GA
Introduction
The adjunct use of tirofiban with heparin has been reported in the literature (1), but there is no consensus on the monitoring of the degrees of platelet glycoprotein (GP) IIb/IIIa blockade during cardiopulmonary bypass (CPB). We have experienced a case where heparin plus tirofiban was used for anticoagulation, and GPIIb/IIIa blockade was monitored with two bed-side coagulation monitors.
Methods
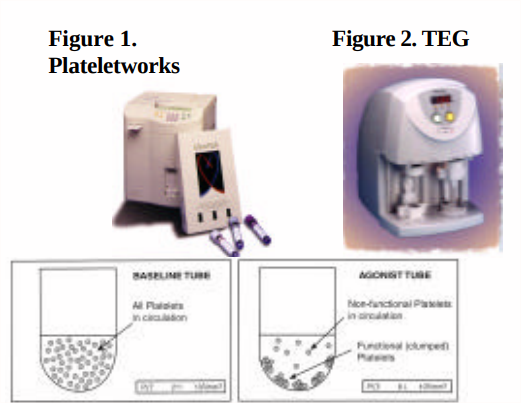
55 year-old patient with a remote history of heparin anaphylaxis, with a negative ELIZA heparin-PF4 assay, was scheduled for an elective coronary bypass surgery. Tirofiban (10 μg/kg) was administered intravenously prior to systemic heparinization, and tirofiban infusion (0.15 μg/kg/min) was continued approximately 60 minutes prior to the estimated discontinuation of CPB. Platelet function was monitored with Plateletworks (Helena Laboratories, Beaumont, Texas, Fig 1) and kaolin-activated thromboelastography (TEG®, Haemoscope, Niles, IL, Fig 2) using the whole blood with heparinase (4 U/mL). Abciximab-modified TEG was also performed.
Results
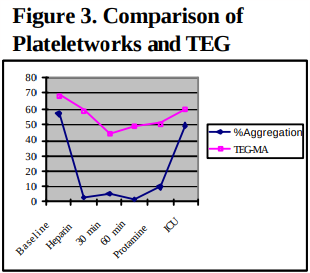
There was a transient drop in the platelet count during CPB. Platelet aggregation induced by ADP (20 μM) was completely suppressed on Plateletworks, whereas the maximum suppression of GPIIb/IIIa receptors was not achieved on TEG (Table & Fig 3). Recovery of platelet count and function were seen by the time of ICU arrival, and the patient did not require hemostatic product transfusion.
Discussion
The fall of platelet count during CPB is partly explained by hemodilution, but subsequent partial recovery (115‡ 176 /mm3 ) suggests that it might be associated with GPIIb/IIIa blockade itself, as eptifibatide is known to cause transient platelet count drop (2,3). Compared to the conventional platelet aggregometry, Plateworks provides results with ease and rapidity. Because tirofiban is a reversible GPIIb/IIIa inhibitor, a recovery of platelet GPIIb/IIIa receptor function may have occurred during TEG evaluation, and lead to a submaximal inhibition. The difference between two devices may also stem from the different activators, ADP (Plateletworks) and endogenous thrombin (TEG) for platelet activation. A further investigation is required for the optimal kind of agonist and its dose for the whole blood-based platelet function tests.
References
- Koster A, Kukucka M, Bach F, et al. Anesthesiology 94; 245-51, 2001
- Hongo RH, Brent BN. American Journal of Cardiology 88:428-31, 2001
- Tanaka KA, Vega JD, Kelly AB, et al. Journal of Thromb Haemost 1:392- 4, 2003
Looking for equipment or accessories for measuring blood platelet levels and other related applications? Browse through our products from Helena Laboratory available on Block Scientific Store today!